J. Carson Smith,1 Kathryn R. Zalewski,1 Robert W. Motl,2 Mark Van Hart,3 Jacob Malzahn1
1University of Wisconsin-Milwaukee; 2University of Illinois at Urbana-Champaign; 3HealthReach Physical Therapy, Brookfield, Wisconsin, USA
Correspondence: J. Carson Smith, Department of Human Movement Sciences, University of Wisconsin-Milwaukee, P.O. Box 413, Milwaukee, WI 53201-0413, USA.
E-mail: jcarson@uwm.edu
Key words: continuing care retirement community, fear of falling, older adults, physical activity accelerometer, self-efficacy, trait anxiety.
Contributions: JCS and KRZ study design, data collection, reduction and analysis, interpretation of results, writing and editing of the manuscript; RW study design, interpretation of results, writing and editing of the manuscript; MVH study design, data collection, interpretation of results, editing of manuscript; JM data collection and reduction.
Acknowledgements: this work was supported by a SEED grant from the College of Health Sciences, University of Wisconsin-Milwaukee to the first author. The authors thank Derek O’Connell for his help with data collection.
Received for publication: 16 February 2010.
Accepted for publication: 10 August 2010.
©Copyright J.C. Smith et al., 2010
Licensee PAGEPress, Italy
Ageing Research 2010; 1:e4
doi:10.4081/ar.2010.e4
AbstractSelf-efficacy for exercise has been shown to be an independent predictor of physical activity (PA) in community dwelling older adults. There is relatively little known, however, regarding the strength and independence of the relationship between self-efficacy and objectively measured PA among residents of continuing care retirement communities (CCRCs). We examined the independent contribution of self-efficacy on PA behavior and assessed whether the explanation of variance in PA behavior was incrementally improved by considering trait anxiety and fear of falling as theoretical impediments to PA. Fifty-two men and women (83.5±5 yrs) residing in one of four CCRCs in metro Milwaukee wore an accelerometer on their ankle for 7 days to measure number of steps per day, the percentage of time spent active and inactive, and moderate and high intensity PA. Self-efficacy for exercise, self-efficacy for overcoming barriers to exercise, trait anxiety, and fear of falling were assessed. Multiple linear regression was utilized to examine the independently explained variance in PA. Exercise self-efficacy significantly and independently explained 13.4% of the variance in number of steps/day (P<0.05). The explanation of variance in moderate intensity activity was incrementally improved when trait anxiety was factored into the model. Overcoming barriers self-efficacy was significantly related to time spent in high intensity activity (r=0.30, P<0.05), but did not significantly and independently explain variance in high intensity PA behavior. Trait anxiety and fear of falling were not identified as significant impediments to PA in CCRC residents. Furthermore, trait anxiety was shown to facilitate, not impede, moderate intensity PA. Self-efficacy for physical activity may serve as a representative target for interventions aimed at increasing physical activity in CCRC residents. |
Continuing care retirement communities (CCRCs) have become an increasingly desirable option as a place to live into old age. The ability to age in place, the sense of community and security, and the availability of social, recreational and physical activity opportunities are important factors for seniors who decide to live in a CCRC.1,2 In particular, the opportunity to remain physically active and socially engaged is viewed by CCRC residents as critical to their ability to remain autonomous into late-life.3,4 The benefits of physical activity (PA) on health and longevity in older adults have been well documented.5,6,7,8,9,10,11 However, most CCRC residents do not meet PA recommendations for older adults,12,13 and activity levels reportedly decline over time in CCRC residents.14 In order to improve the rates of physical activity participation in CCRCs, well-designed interventions that are guided by correlates of PA behavior identified through a solid theoretical framework are needed.15
The well-known role of self-efficacy as both an antecedent and a determinant of physical activity are founded upon the social-cognitive theory developed by Albert Bandura.16,17,18 Social-cognitive theory is based on the view that the persons, their behavior, and the environment mutually interact, termed ‘reciprocal determinism’. As a determinant of behavior, self-efficacy expectations are considered to be an important social-cognitive process. Self-efficacy expectations, defined as the conviction that one can successfully engage in a behavior required to produce a desired outcome, are hypothesized to develop from four primary sources:16 i) performance accomplishments; ii) vicarious experience; iii) verbal persuasion; and iv) emotional arousal. Self-efficacy expectations are distinguished from response-outcome expectations, which are defined as an individual’s estimate that a certain behavior will result in a certain outcome. A strong belief that a certain behavior will produce an outcome will not likely influence behavior, however, unless accompanied by the confidence to perform the behavior. Of note for the current study, emotional arousal and fear reactions are hypothesized to reduce expectations of behavioral success, perhaps through the generation of anticipatory self-arousal in regard to the feared situation. In this case, one might hypothesize PA behavior would be impeded by increased emotional arousal or fear, especially if the fear was heightened while active, such as the fear of falling. On the other hand, as Bandura16 has pointed out, in some situations the cognitive appraisal of one’s arousal might produce behavioral activation rather than behavioral inhibition.19,20
In the context of PA, much work has focused on the role of performance accomplishments, typically defined as the level of past PA behavior, as a source of self-efficacy information due to the relative importance of mastery experiences in the development of self-efficacy.21 Previous work has indicated positive associations between self-efficacy expectations for exercise, outcome expectations for exercise, and current exercise behavior in residents of CCRCs.22 Self-efficacy for PA has been shown to predict maintenance of physical activity behavior22,23,24,25 and has been shown to mediate the effects of improved mood and social support on subjectively measured physical activity behavior among healthy community dwelling older adults.26
Additional factors theorized to be related to exercise behavior, such as mental and physical health status, have been reported to be indirectly related to PA through relationships with self-efficacy expectations and outcome expectations.13 Previous studies in CCRC residents, however, have not considered the role of trait anxiety, which can be defined as the propensity to experience feelings of increased anxiety in various situations,27 and fear of falling28,29 as potential personal or situational impediments to PA behavior.18 Another weakness of past studies of PA behavior in CCRCs has been the use of subjective recall measures of physical activity, which may not accurately reflect actual levels of PA behavior in this population.30
The purpose of this study was to examine the roles of self-efficacy for exercise and self-efficacy for overcoming barriers to exercise on PA behavior measured by an ankle worn accelerometer in older adults living in a CCRC. We also tested the additional roles of trait anxiety and fear of falling as potential impediments to PA behavior. We hypothesized self-efficacy for exercise and self-efficacy for overcoming barriers to exercise would be significantly positively correlated with objectively measured physical activity behavior. We further hypothesized that trait anxiety and fear of falling would be negatively correlated with physical activity behavior. Taken together, we further hypothesized that the explanation of variance in PA behavior would be enhanced by accounting for the incremental increase in the variance explained by trait anxiety and fear of falling after controlling for the variance explained by self-efficacy for exercise and overcoming barriers self-efficacy. This paper reports on data collected as part of a larger study exploring physical activity, physical abilities, mental and physical health status, and social-cognitive variables in older adults.31
Approval for the study was obtained from the Institutional Review Board of the University of Wisconsin-Milwaukee, USA, and written informed consent was obtained from all participants. Sixty participants were recruited from four continuing care retirement communities, providing services and approximately 400 apartments (some >1 resident) to adults aged 55 years and older. These facilities represent two private non-profit religious affiliated institutions, and two private for-profit facilities. All of the facilities were within a 60-mile radius of the University of Wisconsin-Milwaukee, USA. This study included only those individuals who resided in independent or assisted living apartments in the participating CCRCs. Eligible participants were required to self-report walking as their primary means of mobility inside the facility, but were allowed to use an assistive device. Participants were excluded from the analysis if their mini-mental state examination (MMSE)29 score was below 24.
One participant withdrew from the study citing lack of time to complete the initial test battery. One participant was excluded with a MMSE score of 21. Six participants were excluded because they did not provide accelerometer data. After the exclusion of these eight participants, the analyses were based on fifty-two participants who had valid accelerometer data.
Participants were recruited through informational sessions (total attendance of 81 residents), fliers distributed to the residents’ mailboxes and in public places including common dining areas (approximate distribution of 400 fliers), and through word of mouth. Those who were interested were invited to return on a specific date to participate in the study. Each of the CCRCs offered comprehensive rehabilitation services. Participants who required support in order to complete the study surveys could seek assistance from one of the researchers or from individuals employed in the CCRC recreation department.
Participants completed one session of data collection at the CCRC in which they resided and wore an ankle-mounted accelerometer for 7 continuous days. During the 7-day wear period, participants were asked to complete several additional questionnaires at home, which were returned to the investigators one week later, with the accelerometer, at their CCRC. This procedure was followed in order to reduce the burden of completing multiple questionnaires during a single session.
As soon as the written informed consent was provided, participants completed a battery of tests. The tests were administered in the following order: mini-mental state examination (MMSE),31 a healthy history and demographics questionnaire, and the survey of activity and fear of falling in the elderly.32 In addition, though not reported here,28 the physical activity survey in the elderly (PASE),30 the multi-directional reach test34 and six-minute walk test were administered, and comfortable gait speed, and fast gait speed were assessed.35
After these tests were completed, each participant was fitted with a stepwatch activity monitor™ (SAM) (LLC, OrthoCare Innovations, MountLake Terrace, WA, USA), which was worn on the ankle and attached with a small velcro strap. Prior to the end of the initial session, participants were provided with a packet of additional questionnaires and were instructed to complete these questionnaires on their own at home and return them in 7 days at the same location along with the accelerometer. These questionnaires included: the overcoming barriers self-efficacy questionnaire;36 the exercise self-efficacy questionnaire;37 and the trait anxiety inventory.27 Participants were provided with a written reminder regarding the proper wear of the SAM and to complete the questionnaire packet. We contacted each participant by phone on the day prior to their appointment to return the SAM and the questionnaire packet as an additional reminder. At the time the SAM was returned, the researcher helped the participant completing any questionnaires that were not completed. If needed, participants were also called by phone to inquire about missing responses on the questionnaires. Despite these efforts, there were missing data (see Data Analysis).
The SAM is a dual-axis accelerometer designed to count steps in individuals with atypical gait characteristics, including those with atypical or slow gaits, and can be specifically configured based on individual gait characteristics. For the current study, all participants used the same settings: the quick stepping option was set to no, walking speed and leg motion were set to normal, and range of speeds was set to uses a moderate range of speeds. Height settings were customized to each participant. Participants wore the SAM for 7 consecutive days and were instructed to apply the SAM upon waking the first day and to only remove the SAM if it became uncomfortable or interfered with sleep. As the SAM is waterproof, participants were encouraged to wear the SAM during water-based physical activity (e.g., water aerobics). Data collected from the 7-day wear period included total steps, the percentage of time spent inactive, percentage of time spent active, and percentage of active time engaged in moderate and high intensity activities.38 The cut-points we used to define the intensity of activity were based on the work by Coleman and colleagues, which defined low intensity activity as 1-15 steps/min; moderate intensity activity as 16-30 steps/min; and high intensity activity as greater than 30 steps/ min.39
Self-efficacy for exercise was measured using the 6-item exercise self-efficacy questionnaire40 and the 13-item overcoming barriers self-efficacy questionnaire.36 The exercise self-efficacy questionnaire asks for subjective ratings of confidence from 0% (not confident at all) to 100% (highly confident) that the individual could participate in moderate intensity physical activity 20 min per day, three times per week for one to six months. The overcoming barriers self-efficacy questionnaire asks for subjective ratings of confidence from 0% (not confident at all) to 100% (highly confident) that the individual could participate in physical activity three times per week for three months when faced with various potential barriers. Trait anxiety was measured using the state trait anxiety inventory27 and fear of falling was measured using the survey of activity and fear of falling in the elderly scale, with a range from 0 (low fear) to 3 (high fear).32
Means and standard deviations were calculated on all variables. All variables were normally distributed (mean skewness and kurtosis values greater than -1.0 and less than +1.0), with the exception of percent active time in high intensity activity which was positively skewed (skewness = 2.24) and leptokurtic (kurtosis = 5.59). Relationships between indices of stepping behavior (total steps/day, percent active time in moderate and high intensity activity) and self-efficacy for exercise, overcoming barriers self-efficacy, trait anxiety, and fear of falling were examined using Pearson’s product moment correlation. Data were missing for exercise self-efficacy (n=3), fear of falling (n=5), overcoming barriers self-efficacy (n=6) and trait anxiety (n=6) because the forms were not returned to the investigators or were not completed at the initial session. A multiple linear regression analysis was used to examine the incremental prediction of PA behavior. We separately regressed total steps per day, percent of active time spent in moderate intensity activity, and percent of active time spent in high intensity activity on self-efficacy for exercise and over-coming barriers to exercise self-efficacy in Block 1 (model 1) and trait anxiety and fear of falling in Block 2 (model 2, the full model). The mean of each variable was substituted for missing data in the regression analyses and we recognize in advance that this attenuates the standard errors by minimizing variance in the outcomes. Cohen’s f2 was calculated (f2 = R2/1- R2) to estimate the effect size for each regression model, as well as the effect size for the full model that was attributable to the addition of Block 2 (f2A = R2model2 - R2model1/1 - R2model2).41 In accordance with Cohen’s guidelines, f2 values of 0.02, 0.15, and 0.35 were interpreted as small, moderate, and large effects, respectively.41
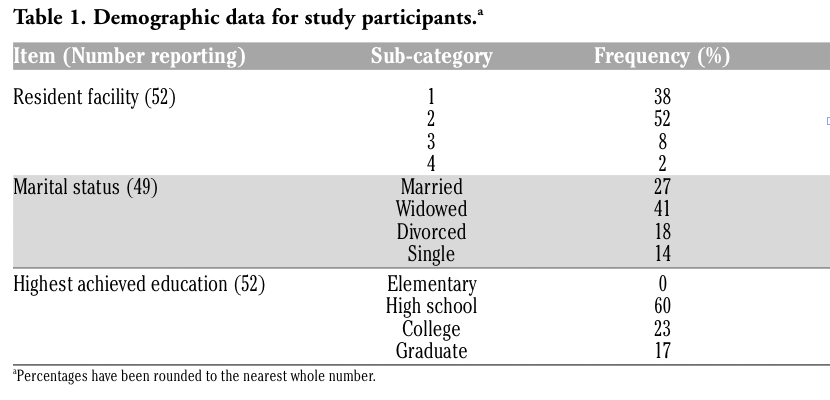
Participant demographic data are presented in Table 1. The sample had a mean age of 84 years, was fairly well-educated, and most were previously or currently married. Participants took an average of three prescription medications, one over the counter medication, and one dietary supplement, consistent with reports of medication usage in older adults in the U.S.42 Table 2 shows the descriptive data for the measures obtained. One participant used an assistive walking device (a “walker”), however this participant was not an outlier and his accelerometer data were nearly identical with the sample means.
Correlations among total number of steps per day, percent of active time in moderate and high intensity physical activity, exercise self-efficacy, overcoming barriers self-efficacy, trait anxiety, and fear of falling and are presented in Table 3. Exercise self-efficacy was the only variable (other than the accelerometer-based outcomes) that significantly correlated with total number of steps per day (r=0.367, P=0.009). A non-significant trend was observed for the correlation between exercise self-efficacy and percentage of time spent in moderate intensity physical activity (r=0.264, P=0.067, two-tailed), while trait anxiety was significantly positively correlated with moderate intensity activity (r=0.292, P=0.049). Overcoming barriers self-efficacy was the only variable significantly correlated with percentage of time spent in high intensity physical activity (r=0.298, P=0.044). Fear of falling was not significantly related to total steps per day, moderate intensity physical activity, or high intensity physical activity behavior.
|
Table 1. Demographic data for study participants.a |
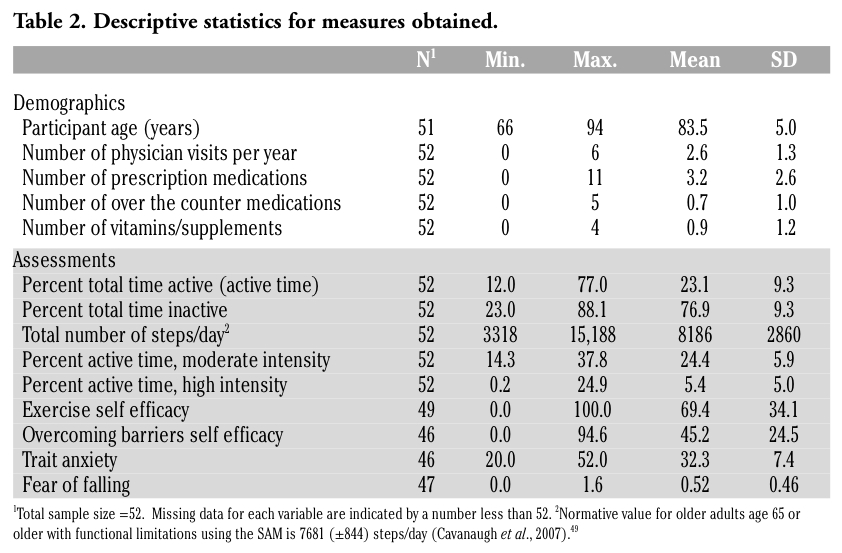 |
Table 2. Descriptive statistics for measures obtained. |
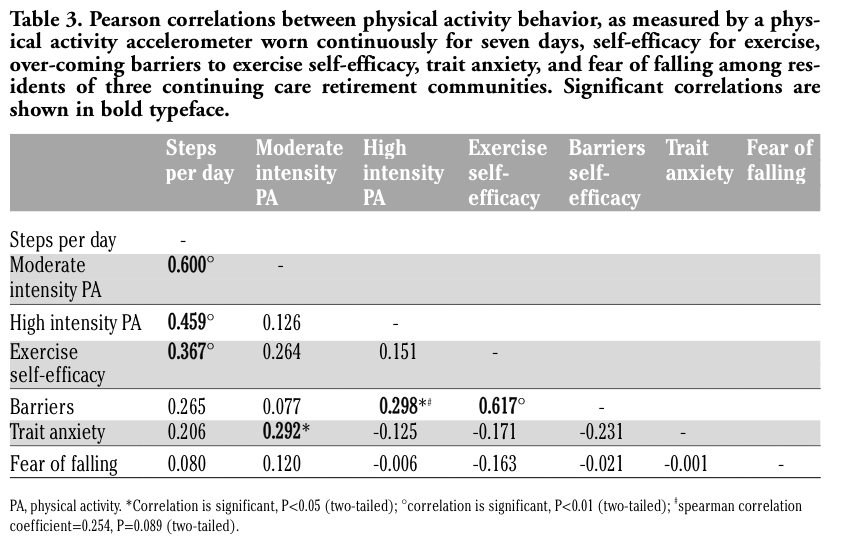 |
Table 3. Pearson correlations between physical activity behavior, as measured by a physical activity accelerometer worn continuously for seven days, self-efficacy for exercise, over-coming barriers to exercise self-efficacy, trait anxiety, and fear of falling among residents of three continuing care retirement communities. Significant correlations are shown in bold typeface. |
A multiple regression analysis indicated that exercise self-efficacy and overcoming barriers self-efficacy explained a significant portion of the variance in total number of steps per day [F(2,49)=3.783, P=0.030; R2 =0.134; f2=0.154], with only exercise self-efficacy as a significant predictor of steps per day (P=0.05).*
*One caveat in the use of a mean substitution approach for missing data is that the standard error may be artificially reduced through the addition of data points that do not vary. However, a comparison of the mean substitution and pairwise exclusion methods did not reveal a substantial decrease in the mean square error of the residual term in either model 1 (a decrease of 0.708%) or model 2 (a decrease of 0.084%). Using the pairwise exclusion of missing cases option, self-efficacy and overcoming barriers self-efficacy explained 13.7% of the variance in total number of steps per day [F(2.38)=3.026, P=0.060), with only exercise self-efficacy as a significant predictor of steps per day (P=0.05). The results for model 2 were similar as well [ΔR2=0.101; ΔF(2,36)=2.377, P=0.107]. The results are nearly identical to the mean substitution method in comparison to a multiple imputation approach (where the missing data are imputed from a conditional distribution based on the observed data). The results for moderate and high intensity activity did not differ substantially between pairwise exclusion and mean substitution options for handling missing cases.
The addition of trait anxiety and fear of falling to the model resulted in a non-significant trend for incremental improvement to the prediction of total number of steps per day [ΔR2 =0.084; ΔF(2,47)=2.611, P=0.084; f2A =0.110]. Using the full model, both exercise self-efficacy (P=0.025, unstandardized β (± SE β) = 33.2 (14.3), standardized β=0.384) and trait anxiety (P=0.045, unstandardized β (± SE β) = 111.1 (53.9), standardized β=0.271) were significant predictors of total number of steps per day [F(4,47)=3.322, P=0.018; f2=0.282].
A multiple regression analysis further indicated that exercise self-efficacy and overcoming barriers self-efficacy did not explain a significant portion of the variance in moderate intensity activity [F(2.49) =1.912, P=0.159; R2 =0.072; f2 =0.078], and exercise self-efficacy showed a non-significant trend as a predictor of moderate intensity activity (P=0.065). The addition of trait anxiety and fear of falling to the model resulted in a significant incremental improvement to the prediction of moderate intensity activity [ΔR2=0.116; ΔF(2.47)=3.373, P=0.043; f2A =0.144]. Using the full model, both exercise self-efficacy (P=0.026, unstandardized β (±SE β)=0.069 (0.030), standardized β=0.387) and trait anxiety (P=0.029, unstandardized β (±SE β) = 0.256 (0.113), standardized β= 0.303) were significant predictors of moderate intensity activity [F(4.47)=2.735, P=0.040; f2=0.233].
A final multiple regression analysis indicated that exercise self-efficacy and overcoming barriers self-efficacy did not explain a significant portion of the variance in high intensity activity [F(2,49) =2.287, P=0112; R2 =0.085; f2 =0.093], and overcoming barriers self-efficacy showed a non-significant trend as a predictor of high intensity activity (P=0.072). The addition of trait anxiety and fear of falling to the model did not result in an incremental improvement to the prediction of high intensity activity [ΔR2 =0.002; f2A=0.003].
The aim of this study was to examine factors that were independently related to objectively measured PA behavior in residents of a CCRC, with a focus on self-efficacy for exercise and self-efficacy for overcoming barriers to exercise as couched with social cognitive theory.16 We also examined the additional variance in PA that may be explained by considering the effects of personal or situational impediments to PA, namely trait anxiety and fear of falling, as suggested more recently by Bandura18 and others.43 We found that self-efficacy for exercise, but not self-efficacy for overcoming barriers to exercise, significantly and independently explained variance in the total number of steps per day. Additionally, we found that accounting for the unique variance explained by trait anxiety significantly increased the amount variance explained in stepping behavior. However, contrary to our hypothesis, higher levels of trait anxiety were independently related to a greater number of steps per day and greater amounts of moderate intensity PA.
Whereas exercise self-efficacy has been shown to be a key factor related to current exercise behavior in healthy older adults, there have been limited reports of this relationship among older adults who live in a CCRC. One previous report utilized individual interviews among CCRC residents to inquire about subjective physical activity behavior13 and reported significant correlations between current physical activity behavior and exercise self-efficacy that were similar in magnitude to the current study. The current study extends these findings by incorporating an objective measure of physical activity behavior through the use of physical activity accelerometers. Importantly, the use of accelerometer-based physical activity monitors permits the categorization of the quality of the physical activity based on the intensity and eliminates subjective bias or poor memory for physical activity as sources of measurement error.
Contrary to our prediction that increased anxiety would be an impediment to being physically active, trait anxiety was independently positively related to total number of steps per day and moderate intensity physical activity, although its addition to the regression models incrementally improved the amount of variance explained only in moderate intensity stepping behavior. This finding is also contrary to reports that a mood disturbance is related to lower levels of PA.21 One possible explanation is that generalized anxiety symptoms may promote physiological arousal and behavioral activation.44 In a large sample of older adults, Li and colleagues reported that worry over health concerns was negatively related to subjectively determined physical activity participation.45 The trait anxiety inventory we employed was not specific to health issues, but is predictive of the level of anxiety one may experience when faced with acute stress.27 It should be noted, however, that the current sample scored within the normal limits for trait anxiety (based on normative data for healthy adults).27 It is plausible that the relationship observed in the present study between trait anxiety and physical activity behavior reflects the tendency of individuals with greater generalized anxiety to show greater patterns of gross motor activation,46 but not necessarily high intensity PA. Our findings do not indicate a relationship between anxiety and higher intensity physical activity, which has been associated with reduction in anxiety in older adults.47
Fear of falling was not related to total physical activity counts or moderate or high intensity activity, and did not independently increase the amount of variance explained in total steps per day or moderate or high intensity PA behavior. This suggests that fear of falling is not a primary consideration of CCRC residents in regard to being physically active. However, this interpretation should be viewed cautiously, as there may have been a sampling bias whereby only those CCRC residents who were interested in physical activity, and had low fear falling in regard to walking, volunteered to participate. It is also plausible that the CCRC built environment may relieve some fear of falling due to the greater number of assistive devices and personnel in place, such as hand railings, proper flooring, fewer staircases and more ramps, and staff people who are available to provide supportive assistance if necessary. In order to better address this issue, future studies should assess the relationships between fear of falling and physical activity among those with both high and low fear of falling and compare these relationships among both CCRC residents and independent community-dwelling older adults.
Interestingly, self-efficacy for overcoming barriers to exercise was the only factor significantly related to high intensity physical activity in these CCRC residents. However, using a regression analysis, overcoming barriers self-efficacy did not significantly explain variance in high intensity PA in our sample. This result should be viewed cautiously, however, as our small sample size may have resulted in a Type II error. If similar small effect sizes (f2=0.09) can be replicated in a larger sample in a future study, this would suggest that confidence, or strategies in place, for overcoming obstacles to being physically active may enhance higher intensity physical activity behavior in CCRC residents. One may speculate that higher intensity activity is also likely to be experienced as more effortful and more physiologically arousing compared to the more commonly performed moderate intensity activity among CCRC residents, and may entail a more goal-oriented and intentional plan to carry out such activity. This view is consistent with Bandura’s theory that those with higher efficacy will be less discouraged, and able to maintain efficacious cognitions, when faced with barriers or impediments to engaging in a health behavior.18 However, we did not assess current physical activity goals or intentions in our sample. This study, nevertheless, extends the work that has been reported regarding PA in CCRC residents by making a distinction between different intensities of PA using an accelerometer. Previous reports of physical activity behavior in CCRC residents have been limited to the subjective report of overall level of physical activity and have not distinguished between the intensity of activity.13 The current findings have important implications, as higher intensity physical activity may confer greater health benefits in older adults.48 Our findings suggest interventions to increase physical activity in CCRC residents that focus on addressing the barriers to being physically active may be an effective method to increase higher intensity physical activity behaviors.
There are several limitations of this study, which assessed relationships among several putative correlates of physical activity behavior, but did not perform an experimental manipulation. Thus, these associations should be viewed with caution, as they do not permit an inference regarding the temporal sequence underlying these relationships. We did not have enough participants to model the possible inter-relationships among these variables using advanced analyses such as covariance modeling. In addition, for some of the measures, some of the participants did not complete the inventory, or did not answer one or more questions.
Despite these weaknesses, the acquisition of accelerometer data among CCRC residents has not been reported previously, and this study adds important information regarding potential targets for future interventions to increase physical activity behavior in CCRCs. As we have previously reported,30 self-reported PA among this sample of CCRC residents did not correlate with steps per day as measured by the activity accelerometer (r=0.073). Future studies should consider using an objective measure of PA, in addition to self-report measures, in a CCRC setting. We have previously reported that this sample of CCRC residents were more physically limited based on tests of physical function compared to normative data.30 Despite their poor performance on tests of physical function (multi-directional reach test; six-minute walk test; comfortable gait speed; fast gait speed) these CCRC residents exhibited greater amounts of physical activity behavior compared to normative values.49 Thus, it is plausible that CCRCs are supportive of physical activity behavior, perhaps through increased social support3 or other supportive features, even in the face of physical functional limitations.
In summary, among older adults living in a CCRC, objectively measured number of steps per day and moderate intensity physical activity behavior were independently explained by exercise self-efficacy, and the amount of variance explained was increased by considering the level of trait anxiety. Trait anxiety, however, was related to greater PA behavior, and was not found to be an impediment to being physically active. Only high intensity physical activity was weakly though significantly related to self-efficacy for overcoming barriers to exercise. Taken together, these data suggest interventions aimed at enhancing self-efficacy for physical activity and providing strategies for overcoming barriers to being physically active may be effective at promoting physical activity among residents of CCRCs. Future studies should determine the independent influence of a greater breadth of personal, situational and environmental impediments, as well as facilitative factors, related to physical activity behavior in CCRC residents.
1. Cutchin MP, Marshall VW, Aldrich R. Moving to a continuing care retirement community: occupations in the therapeutic landscape process. J Cross Cult Gerontol 2010;25:117-32.[PubMed]
2. Krout JA, Oggins J, Holmes HH. Patterns of service use in a continuing care retirement community. Gerontologist 2000;40: 698-705.[PubMed]
3. Heisler EG, Evans W, Moen P. Health and social outcomes of moving to a continuing care retirement community. Journal of Housing for the Elderly 2004;18:5-24.[FULLTEXT]
4. Shippee TP. “But I am not moving”: residents' perspectives on transitions within a continuing care retirement community. Gerontologist 2009;49:418-27.[PubMed]
5. Bembom O, van der Laan M, Haight T, Tager I. Leisure-time physical activity and all-cause mortality in an elderly cohort. Epidemiology 2009;20:424-30.[PubMed]
6. Haapanen N, Miilunpalo S, Vuori I, et al. Characteristics of leisure time physical activity associated with decreased risk of premature all-cause and cardiovascular disease mortality in middle-aged men. Am J Epidemiol 1996;143:870-80.[PubMed]
7. Kampert JB, Blair SN, Barlow CE, et al. Physical activity, physical fitness, and all-cause and cancer mortality: a prospective study of men and women. Ann Epidemiol 1996;6:452-7.[PubMed]
8. LaFontaine T, Dabney S, Brownson R, Smith C. The effect of physical activity on all cause mortality compared to cardiovascular mortality: a review of research and recommendations. Mo Med 1994;91:188-94.[PubMed]
9. Paffenbarger RS Jr, Hyde RT, Wing AL, Hsieh CC. Physical activity, all-cause mortality, and longevity of college alumni. N Engl J Med 1986;314:605-13.[PubMed]
10. Paffenbarger RS Jr, Lee IM. Intensity of physical activity related to incidence of hypertension and all-cause mortality: an epidemiological view. Blood Press Monit 1997;2:115-23.[PubMed]
11. Steffen-Batey L, Nichaman MZ, Gof, DC, et al. Change in level of physical activity and risk of all-cause mortality or reinfarction: The Corpus Christi Heart Project. Circulation 2000;102:2204-9.[PubMed]
12. Nelson ME. Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc 2007;39:1435-45.[PubMed]
13. Resnick B. A prediction model of aerobic exercise in older adults living in a continuing-care retirement community. J Aging Health 2001;13:287-310.[PubMed]
14. Resnick B. A longitudinal analysis of efficacy expectations and exercise in older adults. Res Theory Nurs Pract 2004;18:331-44.[PubMed]
15. Rosenberg D, Kerr J, Sallis JF, et al. Feasibility and outcomes of a multilevel place-based walking intervention for seniors: a pilot study. Health Place 2009; 15:173-9.[PubMed]
16. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev 1977;84:191-215.[FULLTEXT]
17. Bandura A. Self-Efficacy: The Exercise of Control. 1997, Freeman, New York, NY, USA.[PubMed]
18. Bandura A. Health promotion by social cognitive means. Health Educ Behav 2004;31:143-64.[PubMed]
19. Lang PJ. The emotion probe. Studies of motivation and attention. Am Psychol 1995; 50:372-385.[PubMed]
20. Weiner B. Theories of motivation. 1972, Markham,Chicago, IL, USA.
21. Trost SG, Owen N, Bauman AE, et al. Correlates of adults' participation in physical activity: review and update. Med Sci Sports Exerc 2002;34:1996-2001.[PubMed]
22. Resnick B, Nigg C. Testing a theoretical model of exercise behavior for older adults. Nurs Res 2003;52:80-8.[PubMed]
23. Booth ML, Owen N, Bauman A, et al. Social-cognitive and perceived environment influences associated with physical activity in older Australians. Prev Med 2000;31:15-22.[PubMed]
24. Burton LC, Shapiro S, German PS. Determinants of physical activity initiation and maintenance among community-dwelling older persons. Prev Med 1999;29: 422-30.[PubMed]
25. Resnick B. Testing a model of exercise behavior in older adults. Res Nurs Health 2001;24:83-92.[PubMed]
26. McAuley E, Jerome GJ, Marquez DX, et al. Exercise self-efficacy in older adults: social, affective, and behavioral influences. Ann Behav Med 2003;25:1-7.[PubMed]
27. Spielberger CD, Gorsuch RL, Lushene PR, et al. Manual for the State-Trait Anxiety Inventory. 1983, Consulting Psychologists Press, Inc, Palo Alto, CA, USA.
28. Li F, Fisher KJ, Harmer P, et al. Fear of falling in elderly persons: association with falls, functional ability, and quality of life. J Gerontol B Psychol Sci Soc Sci 2003;58: P283-90.[PubMed]
29. Lian WM, Gan GL, Pin CH, et al. Correlates of leisure-time physical activity in an elderly population in Singapore. Am J Public Health 1999;89:1578-80.[PubMed]
30. Zalewski KR, Smith JC, Malzahn J, et al. Measures of physical ability are unrelated to objectively measured physical activity behavior in older adults residing in continuing care retirement communities. Arch Phys Med Rehabil 2009;90:982-6.[PubMed]
31. Folstein MF, Folstein SE, McHugh PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-98.[PubMed]
32. Lachman ME, Howland J, Tennstedt S, et al. Fear of falling and activity restriction: the survey of activities and fear of falling in the elderly (SAFE). J Gerontol B Psychol Sci Soc Sci 1998;53:P43-50.[PubMed]
33. Washburn RA, Smith KW, Jette AM, Janney CA. The Physical Activity Scale for the Elderly (PASE): development and evaluation. J Clin Epidemiol 1993;46:153-62.[PubMed]
34. Duncan PW, Weiner DK, Chandler J, Studenski S. Functional reach: a new clinical measure of balance. J Gerontol 1990;45:M192-97.[PubMed]
35. Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys Ther 2002;82:128-37.[PubMed]
36. McAuley E. Self-efficacy and the maintenance of exercise participation in older adults. J Behav Med 1993;16:103-13.[PubMed]
37. McAuley E. The role of efficacy cognitions in the prediction of exercise behavior in middle-aged adults. J Behav Med 1992;15: 65-88.[PubMed]
38. Foster RC, Lanningham-Foster LM, Manohar C, et al. Precision and accuracy of an ankle-worn accelerometer-based pedometer in step counting and energy expenditure. Prev Med 2005;41:778-83.[PubMed]
39. Coleman KL, Smith DG, Boone DA, et al. Step activity monitor: long-term, continuous recording of ambulatory function. J Rehabil Res Dev 1999;36:8-18.[PubMed]
40. McAuley E. The role of efficacy cognitions in the prediction of exercise behavior in middle-aged adults. J Behav Med 1992;15: 65-88.[PubMed]
41. Cohen J. Statistical power analysis for the behavioral sciences, 2nd ed. 1988, Erlbaum, Hillsdale, NJ, USA.
42. Grymonpre RE, Hawranik PG. Rural residence and prescription medication use by community-dwelling older adults: a review of the literature. J Rural Health 2008;24: 203-9.[PubMed]
43. Morris KS, McAuley E, Motl RW. Self-efficacy and environmental correlates of physical activity among older women and women with multiple sclerosis. Health Educ Res 2008;23:744-52.[PubMed]
44. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition - Text Revision (DSMIV-TR). 2000. American Psychiatric Association, Arlington, VA, USA.[FULLTEXT]
45. Li KK, Cardinal BJ, Vuchinich S. Health worry, physical activity participation, and walking difficulty among older adults: a mediation analysis. Res Q Exerc Sport 2009;80:12-21.[PubMed]
46. Roth WT, Doberenz S. Dietel A, et al. Sympathetic activation in broadly defined generalized anxiety disorder. J Psychiatr Res 2008;42:205-12.[PubMed]
47. Cox RH. Thomas TR, Hinton PS. Donahue OM. Effects of acute 60 and 80% VO2max bouts of aerobic exercise on state anxiety of women of different age groups across time. Res Q Exerc Sport 2004;75:165-75.[PubMed]
48 Janssen I, Jolliffe C J. Influence of physical activity on mortality in elderly with coronary artery disease. Med Sci Sports Exerc 2006;38:418-7.[PubMed]
49. Cavanaugh JT, Coleman KL, Gaines et al. Using step activity monitoring to characterize ambulatory activity in community-dwelling older adults. J Am Geriatr Soc 2007;55:120-4.[PubMed]
[TOP]